

MCC in Oral Suspensions has become one of the most important technologies for improving suspension stability in modern pharmaceutical development. Oral suspensions play a critical role in pharmaceutical manufacturing, especially for pediatric and geriatric patients. Because children cannot swallow tablets and elderly patients often have dysphagia, oral liquid suspensions provide the only viable option. Moreover, patients who need flexible dose titration rely on these formulations. This challenge becomes more serious in antibiotic oral suspension formulation, because high API loading accelerates sedimentation. Nevertheless, oral suspensions remain technically challenging to stabilize. Therefore, choosing the right oral liquid suspension excipient ensures long-term physical stability.
The core problem is physics. Drug particles in a suspension are denser than the surrounding liquid medium. Gravity pulls them downward — continuously, inevitably. Without an effective pharmaceutical suspension stabilizer, a chemically stable product still separates into a watery supernatant and dense sediment. Moreover, this sediment can become irreversible at the bottom of the bottle. Therefore, achieving meaningful suspension stability improvement requires more than simply increasing viscosity. As a result, inconsistent dosing occurs, reducing patient confidence and risking regulatory failure.
This is precisely why microcrystalline cellulose oral suspension technology has become the gold standard approach for stabilizing oral pharmaceutical liquids. When formulators use an MCC CMC oral suspension system, they achieve excellent suspension stability, redispersibility, and mouthfeel. In contrast, traditional gums and thickeners cannot deliver the same performance.
In this guide, we explain how MCC in oral suspensions works. We also show why it outperforms alternatives and how formulators can use it correctly. Finally, we discuss the fastest-growing application areas and market demand.
In a typical microcrystalline cellulose oral suspension, MCC functions as a pharmaceutical suspension stabilizer that prevents sedimentation, improves redispersibility, and maintains dose uniformity.
MCC is widely used as a suspending agent for oral suspensions because it prevents sedimentation and improves redispersibility.
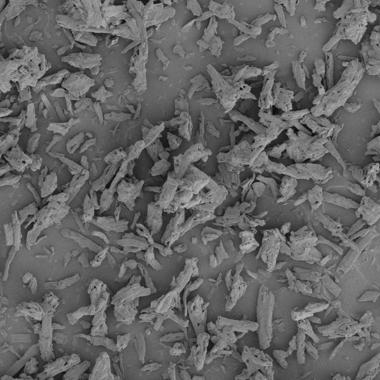
Microcrystalline Cellulose is a purified, partially depolymerized cellulose derived from natural plant fiber sources. In solid dosage forms, MCC is best known as the premier direct compression excipient and tablet binder — and for good reason. But its role in oral liquid suspension formulation is equally important and increasingly recognized by formulators worldwide.In modern pharmaceutical development, the MCC CMC suspension system is considered the industry benchmark for oral liquid suspension stabilization.
Most conventional suspension stabilizers — xanthan gum, HPMC, sodium CMC, sodium alginate — work by increasing bulk viscosity. The logic is straightforward: a thicker liquid slows particle settling. The problem is simple: high-density API suspensions need viscosity to prevent sedimentation. However, this often makes the product too thick to pour, unpleasant in the mouth, and hard for pediatric or elderly patients to swallow.
Compared with traditional gums, MCC acts as a multifunctional oral liquid suspension excipient. It stabilizes particles through structure rather than viscosity alone.
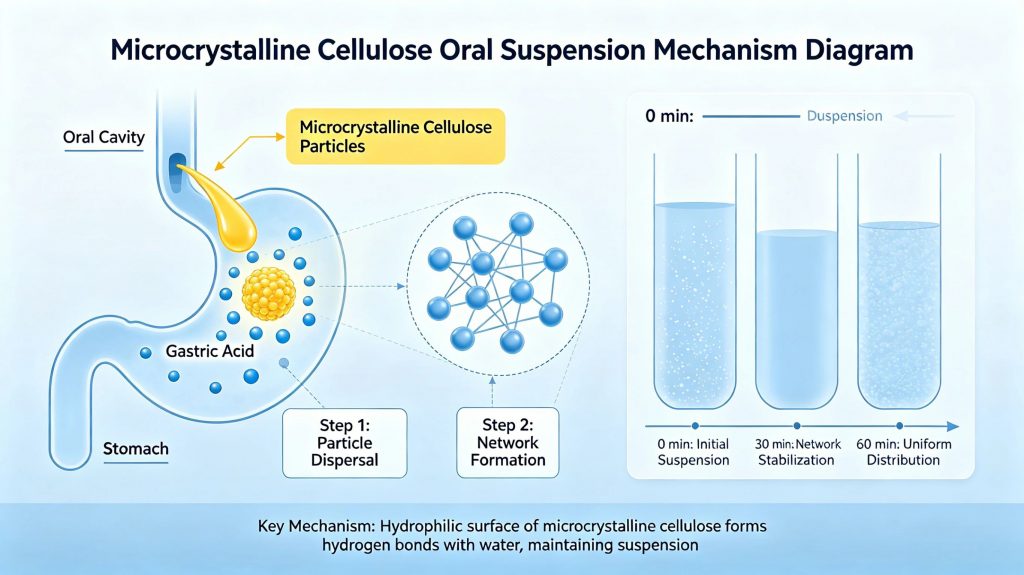
MCC works differently. When formulators disperse it in water, especially in its co-processed form combined with CMC, MCC does not merely dissolve or thicken. Instead, it forms a three-dimensional colloidal gel network throughout the liquid.
This network physically traps API particles and holds them in suspension through structural support rather than viscosity alone. As a result, the suspension pours freely, feels smooth, and resists sedimentation more effectively than any viscosity-based system.
Not all MCC grades perform equally in liquid systems. Therefore, formulators select grades carefully because grade selection determines network density, viscosity contribution, and suspension efficiency. This makes it one of the most critical decisions in oral suspension formulation development.
Commonly used grades include:
MCC/CMC co-processed systems — formulators use them as the industry standard for oral suspension stabilization.
ACTA-591 type — contains approximately 89% MCC and 11% CMC. It is the most widely referenced suspension grade globally.
ACTA-611 type — contains approximately 85% MCC and 15% CMC. It provides higher CMC content and increased viscosity.
Customized MCC suspension stabilizer blends — formulators design these blends for specific API density, target viscosity, or reconstitution needs.
Each grade shows a distinct viscosity profile, gel strength, and suspension efficiency. In practice, grade selection depends on formulation requirements, from low-viscosity systems to high-density API challenges.
Selecting the appropriate MCC CMC suspension system often matters more than simply increasing viscosity.
Low viscosity suspension systems are used for APIs with low bulk density and good wettability. In these systems, MCC/CMC mainly prevents sedimentation rather than builds viscosity.
These systems are common in pediatric oral suspensions, thin antacid liquids, and some nutritional products.
For these uses, formulators select ACTA-591 (89% MCC / 11% CMC). They use it at a low level, usually 0.5–0.8% w/v. This level forms a weak colloidal network. And it still keeps good pourability.
The lower CMC content reduces chain entanglement. So the system stays light and easy to pour. It also improves dose accuracy with oral syringes.
Formulators should check final viscosity at rest. The system must prevent sedimentation. And it must still allow easy shaking and redispersion. A small yield stress is ideal. It stops settling but avoids thick texture.
Medium viscosity systems are the most common oral suspension type. They include antibiotics, analgesics, and corticosteroids for pediatric and adult use.
These formulations need a stronger colloidal network. They must support moderate API density. And they must meet longer shelf-life requirements.
Two grade options work well in this range:
ACTA-591 at 0.8–1.2% w/v is suitable when moderate viscosity is enough. It gives a lighter texture and smooth flow.
ACTA-611 at 0.6–1.0% w/v is preferred when higher structure is needed. Its higher CMC content (15%) increases chain entanglement. So it builds stronger gel strength at lower dose.
For dry suspensions, ACTA-591 is used at 1.5–2.0% w/w in the blend. The system must hydrate fast and fully. So formulators should test hydration under real use conditions. These include water volume, bottle shape, and shaking method.
High-density APIs create stronger formulation challenges. Examples include barium sulfate, bismuth subsalicylate, zinc oxide, and other mineral actives.
Sedimentation increases with particle size and density difference. This follows Stokes’ law. So even stable systems can fail at normal polymer levels.
For these cases, ACTA-611 is preferred. A higher CMC blend can also be used. Formulators apply 1.5–2.0% w/v at the upper range.
Higher CMC increases yield stress. It also improves thixotropic recovery. So the structure rebuilds after shaking or pouring. This helps keep dose uniform during use.
Formulators can also combine strategies:
They reduce particle size through micronization. This slows sedimentation.
They adjust medium density with co-solvents or high sucrose levels. This reduces settling force.
They also combine MCC/CMC with xanthan gum. This creates a stronger synergistic network.
Stability tests must run long term. They should measure sedimentation volume over time. They should also test redispersibility. And they must test both upright and inverted storage.
Qualifying a new MCC/CMC supplier involves parallel streams of regulatory, analytical, and functional evaluation. The following steps define a defensible qualification process:
Confirm that the supplier holds a current Drug Master File (DMF) or equivalent regulatory filing in the target markets (US FDA, EMA, NMPA, etc.). Review the DMF for completeness of process description, impurity controls, and specification alignment with Ph. Eur., USP/NF, or JP monographs as applicable. Ensure the excipient is manufactured under ICH Q7-aligned GMP conditions.
Establish a side-by-side specification comparison between the incumbent and candidate grades, covering: assay (MCC and CMC content), viscosity, loss on drying, pH, heavy metals, microbial limits, and particle size. Any specification gap must be assessed for formulation impact before proceeding.
Prepare representative suspension batches using the candidate MCC/CMC at the same concentration used with the current grade. Compare viscosity profiles (low and high shear), sedimentation volume ratio at defined time points, redispersibility, and zeta potential where applicable. Testing should be conducted in the actual product formulation matrix, not in water alone.
Place comparability batches on accelerated stability (40°C/75% RH, minimum 3 months) alongside current-grade reference batches. Key endpoints: viscosity retention, sedimentation behavior, pH stability, and API assay. A significant divergence in stability profile between incumbent and candidate grades at this stage disqualifies the alternative regardless of initial functional comparability.
In most jurisdictions, a change of excipient supplier requires a post-approval change submission (Type IA/IB in EU; Annual Report or Prior Approval Supplement in US, depending on impact assessment). Prepare the regulatory strategy in parallel with technical qualification to avoid timeline delays upon successful qualification.
Completing all five steps before commercial supply commitment protects formulation integrity, ensures regulatory compliance, and establishes the data package needed to defend the change in any subsequent inspection or query.
The most effective and commercially proven MCC CMC suspension system is the co-processed MCC/CMC technology. In this format, MCC and sodium carboxymethylcellulose are intimately combined during manufacturing — not simply blended as separate powders. This co-processing creates a material where CMC coats individual MCC microfibrils, enabling rapid, uniform hydration and consistent colloidal network formation upon dispersion in water.
The practical advantage is significant: co-processed MCC/CMC disperses more reliably, hydrates more completely, and produces more reproducible suspension performance batch-to-batch compared to physical blends of the two components. This is why co-processed grades such as Avicel RC-591 type systems have become the industry reference standard for pharmaceutical suspension stabilizer applications in oral liquid formulations.
| Property | Value | Formulation Relevance |
|---|---|---|
| Particle size | 20–200 µm (grade-dependent) | Controls network density and suspension efficiency |
| Ionic character | Non-ionic | Broad API and excipient compatibility |
| pH stability | 3–11 | Consistent performance across acidic and neutral suspensions |
| Water dispersibility | Excellent | Rapid network formation upon hydration |
| Regulatory status | USP / EP / JP | Global market access without re-qualification |
| Inertness | Chemically inert | No interaction with APIs or preservatives |
To understand why MCC suspension stabilizer systems are so valuable, you first need to understand the physics of what happens when suspension formulation goes wrong.
Every insoluble API particle in a liquid suspension is subject to Stokes’ Law — one of the most fundamental equations in pharmaceutical suspension science. Stokes’ Law states that the rate of particle sedimentation is directly proportional to the square of the particle radius and the density difference between the particle and the surrounding medium, and inversely proportional to the viscosity of the medium. Effective particle immobilization is the key to long-term suspension stability improvement.Written simply:
Sedimentation rate ∝ (particle radius)² × (particle density − medium density) / medium viscosity
In practical formulation terms, this means three things: larger particles settle faster than smaller ones — dramatically so, since the relationship is squared. Denser APIs settle faster in low-density aqueous vehicles. And low-viscosity liquids offer far less resistance to settling than thicker ones. For a typical pharmaceutical oral suspension containing a dense, poorly soluble API in an aqueous vehicle, all three factors work against stability simultaneously.
Particle size is the single most powerful lever available to formulators trying to control sedimentation — because its effect on settling rate is exponential, not linear. Reducing the mean particle diameter of an API from 100 µm to 10 µm reduces the sedimentation rate by a factor of 100. This is why micronization of APIs intended for suspension formulation is standard practice in pharmaceutical manufacturing.
However, micronization alone does not solve the sedimentation problem. Smaller particles settle more slowly, but they also have greater surface energy and a stronger tendency to aggregate — forming larger secondary particles that settle just as rapidly as the original unmicronized material. Without an effective suspending agent to stabilize individual particles and prevent aggregation, micronization provides only temporary benefit.
This is exactly where MCC/CMC colloidal suspension systems deliver their greatest value: by forming a structural network that physically prevents both primary particle settling and secondary aggregate formation, regardless of the API particle size distribution.
Poor sedimentation control is not merely a manufacturing quality issue — it is a direct patient safety concern. The consequences cascade from the formulation laboratory through to the patient at the bedside:
| Problem | Clinical / Commercial Impact |
|---|---|
| Non-uniform drug distribution | Variable dose per administration — regulatory failure risk |
| Hard cake formation | Irreversible sediment that cannot be redispersed — product rejection |
| Poor redispersibility | Patients cannot reliably resuspend — dosing errors |
| Unacceptable appearance | Consumer rejection; perceived poor quality |
| Stability test failure | Batch rejection; costly reformulation |
| Aggregation of particles | Accelerated sedimentation; altered dissolution rate |
Consider the clinical stakes in context. In antibiotic oral suspension formulation, non-uniform sedimentation may cause the first doses to contain less API than intended. In adult patients this is a serious concern.
For pediatric oral suspensions, where dosing is weight-based and therapeutic windows for many antibiotics are narrow, failing to achieve redispersibility creates a direct patient safety risk.
Redispersibility — the ability of a settled suspension to return to a uniform, homogeneous state after gentle shaking — represents one of the most clinically and regulatorily important quality attributes of any oral suspension product. Yet formulators often underweight it during early development.
The reason redispersibility matters so strongly is behavioral: patients and caregivers do not shake medication bottles as rigorously as formulation scientists do in the lab. Real-world shaking varies — sometimes vigorous, sometimes gentle, sometimes skipped entirely. If a suspension needs 60 seconds of hard shaking to redisperse, caregivers routinely deliver non-uniform doses in practice, regardless of label instructions.
Regulatory agencies acknowledge this risk. ICH guidelines require testing suspension redispersibility as part of physical stability evaluation. FDA and EMA also expect formulators to show adequate redispersion under conditions that mimic actual patient use rather than ideal laboratory conditions.
This is why developers carefully evaluate suspending agents for oral liquids. MCC/CMC colloidal systems provide a clear advantage: they consistently redisperse to homogeneity within seconds of gentle shaking, even after months of storage. This performance offers meaningful clinical and commercial benefits over alternatives that rely solely on viscosity.
What makes MCC in oral suspensions fundamentally different from conventional thickeners is its mechanism of action. Traditional suspending agents — xanthan gum, HPMC, sodium alginate — work primarily by increasing bulk viscosity. Higher viscosity slows particle sedimentation. The problem: the level of viscosity needed to adequately prevent sedimentation in a high-density API suspension often produces a product that is too thick to pour, too viscous to dose accurately, and unpleasant in the mouth.The success of a microcrystalline cellulose oral suspension depends on the unique colloidal network formed by hydrated MCC and CMC particles
MCC takes a completely different approach.
The MCC colloidal suspension mechanism — step by step:
Upon dispersion in water, MCC microfibrils hydrate and interact with CMC chains. The CMC component stabilizes MCC particle surfaces and promotes uniform dispersion throughout the liquid.
Hydrated MCC particles form physical junction points, creating a continuous three-dimensional colloidal network throughout the suspension medium. This network has measurable yield stress — it resists deformation under low applied force (such as gravity acting on settling particles) but flows readily under higher shear (such as shaking or pouring).
API particles become physically immobilized within the colloidal network. The network’s yield stress exceeds the gravitational force acting on individual particles — suspending them in place without requiring high bulk viscosity.
When the bottle is shaken (high shear), the network breaks down temporarily and the suspension flows freely. When shaking stops, the network reforms rapidly — re-entrapping particles before significant sedimentation can occur.
Any minor sedimentation that occurs during extended storage remains loose and unconsolidated — easily redispersed by gentle shaking. This is the critical difference between MCC-stabilized suspensions and those relying on viscosity alone, where sediment can compact into hard, irreversible cakes.
This thixotropic colloidal mechanism is why MCC CMC suspension systems consistently outperform conventional thickeners in both suspension stability and patient-critical parameters like pourability, mouthfeel, and dosing accuracy.
A common question among formulators new to MCC oral suspension technology is: why not use MCC alone? The colloidal network mechanism sounds compelling — so why does virtually every pharmaceutical suspension stabilizer application combine MCC with sodium carboxymethylcellulose rather than using MCC as a standalone excipient?
The answer lies in a practical limitation of MCC’s behavior in aqueous systems. While MCC microfibrils have an outstanding capacity to form three-dimensional colloidal networks once properly dispersed, getting them to that dispersed state is the challenge. MCC particles in water tend to aggregate and clump during hydration — particularly under the mixing conditions typical of pharmaceutical liquid manufacturing. Without a dispersing and hydrating aid, MCC hydrates unevenly, leaving poorly dispersed clusters that contribute neither network structure nor suspension performance. The result is batch-to-batch inconsistency and unpredictable suspension stability — unacceptable in pharmaceutical manufacturing where reproducibility is a regulatory requirement.
On the other side of the equation, sodium carboxymethylcellulose alone faces the fundamental limitation shared by all viscosity-based suspending agents: it can only slow sedimentation by thickening the medium, not by structurally immobilizing particles.
To achieve meaningful sedimentation control with CMC alone, concentrations must be high enough to produce a viscosity that resists particle settling under gravity. At those concentrations, the resulting suspension is typically too viscous to pour accurately, produces a thick, slimy mouthfeel that patients — especially children — reject, and creates manufacturing challenges including difficult mixing, air entrapment, and poor dose uniformity during filling. CMC alone also tends to produce hard, difficult-to-redisperse sediment upon prolonged storage — precisely the failure mode that makes a suspension clinically unreliable.
The answer is synergy. Each component directly addresses the other’s core limitation — producing a combined system whose performance far exceeds what either excipient achieves independently.
MCC provides the structural colloidal network that physically entraps and immobilizes API particles. CMC provides the hydration and dispersibility that allows MCC to form that network uniformly and reproducibly. Together, they create a suspension stabilizer system that delivers both structural particle entrapment and controlled viscosity — at concentrations low enough to maintain acceptable pourability and mouthfeel.
| Function | MCC Contribution | CMC Contribution |
|---|---|---|
| Network structure | ✓✓ Primary | Supporting |
| Hydration / dispersibility | Supporting | ✓✓ Primary |
| Viscosity development | Moderate | ✓✓ Primary |
| Particle entrapment | ✓✓ Primary | Supporting |
| Mouthfeel | ✓✓ Creamy | Smoothing |
| Stability | ✓✓ Long-term | Short-term |
| Redispersibility | ✓✓ Primary | Supporting |
| Manufacturing consistency | Supporting | ✓✓ Primary |
The practical outcome: an MCC/CMC suspension system suspends particles more effectively, at lower total polymer concentrations, with better mouthfeel and redispersibility, than either component alone — or than most competing single-excipient systems.
The final evolution of this synergistic system is co-processing — and it represents a meaningful performance upgrade over simply blending MCC and CMC powders together as separate raw materials.
In a physical blend, MCC and CMC particles remain as discrete entities. During manufacturing, they hydrate at different rates and may not achieve intimate contact until mixing is well advanced. The result is variable network formation and batch-to-batch performance inconsistency that creates real challenges for process validation.
In a co-processed grade — such as Avicel RC-591 type systems — CMC is intimately associated with individual MCC microfibrils during the manufacturing process itself. CMC effectively coats MCC particle surfaces, enabling immediate, uniform hydration of MCC upon contact with water. The colloidal network forms faster, more completely, and more reproducibly than any physical blend can achieve.
The practical manufacturing advantages are substantial: shorter hydration times, more consistent viscosity development, more reliable suspension performance across batches, and a simpler manufacturing process requiring fewer processing steps and less operator-dependent mixing judgment.
For pharmaceutical suspension stabilizer applications where both performance and manufacturing reproducibility are non-negotiable — which in regulated pharmaceutical production means every application — co-processed MCC/CMC grades are the most efficient and reliable solution available.
How does MCC perform against the other suspending agents for oral suspensions commonly used in pharmaceutical manufacturing? Understanding where MCC excels — and where alternatives may be considered — is essential for making confident, science-based excipient decisions.
Xanthan gum is probably the most widely used alternative to MCC/CMC in pharmaceutical oral suspensions, and it does provide real suspension performance benefits.
Its pseudoplastic rheology helps control sedimentation effectively, and it maintains good flow under shear while building viscosity at rest. So it supports acceptable physical stability in many oral liquid formulations.
It also has broad global regulatory acceptance across pharmaceutical and food applications, which makes it a convenient formulation option in many development programs.
However, xanthan gum’s critical weakness is mouthfeel. At the concentrations required for effective suspension stabilization, xanthan gum produces a distinctly slimy, stringy texture that a significant proportion of patients — particularly children — find unacceptable. In pediatric oral suspension formulation, palatability is not a secondary consideration. It directly determines whether a child accepts the medication at all. A suspension with outstanding physical stability that a child refuses to swallow has failed its primary clinical purpose.
MCC/CMC systems consistently outperform xanthan gum on redispersibility as well. Xanthan gum-stabilized suspensions tend to form moderately cohesive sediments that require more vigorous shaking to redisperse compared to the loose, easily resuspended sediments characteristic of MCC-based formulations.
Hydroxypropyl methylcellulose is an excellent film-forming and controlled-release polymer, and it provides moderate viscosity-based suspension support in oral liquid formulations. However, HPMC functions purely as a thickener in suspension applications — it has no capacity to form the colloidal structural network that gives MCC/CMC its superior particle entrapment performance.
At viscosity levels where HPMC provides adequate sedimentation control, its mouthfeel is smooth and generally acceptable — a genuine advantage over xanthan gum. But sedimentation control and redispersibility both fall short of MCC/CMC performance, particularly in high-density API suspensions or formulations with high particle loading. For standard viscosity applications and low-density APIs, HPMC may be a viable alternative; for demanding suspension stabilization requirements, MCC/CMC is the stronger choice.
Sodium alginate offers moderate thickening and provides some suspension support, but it delivers a more limited performance profile compared with MCC/CMC in several critical formulation aspects.
Its effective pH range is approximately 5–10, so it excludes many acidic suspension systems where key antibiotic and antifungal APIs show optimal stability.
In addition, its API compatibility is lower than MCC because of its ionic nature. It can interact with cationic APIs and with excipients containing divalent cations. As a result, it may trigger gelling, precipitation, or even viscosity instability in certain formulations.
Redispersibility is moderate at best, and caking tendency is higher than MCC/CMC systems. For most pharmaceutical suspension applications, sodium alginate represents a functional compromise rather than a performance solution.
Sodium CMC alone — without the co-processed MCC component — has historically been one of the most common suspension stabilizers in pharmaceutical oral liquids, and it remains widely used in cost-sensitive formulations.
However, as noted earlier, CMC alone depends entirely on viscosity to control sedimentation. This reliance creates a known failure mode: CMC-only suspensions tend to cake heavily, redisperse poorly after extended storage, and require high polymer concentrations.
These high concentrations can negatively affect mouthfeel and pourability, reducing patient compliance and overall product performance.
In direct head-to-head stability comparisons, MCC/CMC co-processed systems consistently show lower sedimentation rates, better redispersibility, and lower caking scores than equivalent concentrations of sodium CMC used alone.
These differences arise because the MCC/CMC system builds a true three-dimensional network, rather than relying only on viscosity. As a result, it maintains structure more effectively during storage and use.
For any application that requires long-term suspension stability and reliable redispersibility in real patient use, co-processed MCC/CMC provides a measurably superior option.
| Property | MCC/CMC | Xanthan Gum | Sodium Alginate | HPMC | Sodium CMC Alone |
|---|---|---|---|---|---|
| Suspension efficiency | ✓✓ Excellent | Good | Moderate | Moderate | Moderate |
| Sedimentation control | ✓✓ Excellent | Good | Moderate | Moderate | Moderate |
| Redispersibility | ✓✓ Excellent | Moderate | Moderate | Moderate | Poor |
| Mouthfeel | ✓✓ Creamy/smooth | Slimy | Thick/gummy | Smooth | Slimy |
| API compatibility | ✓✓ Excellent | Good | Moderate | Good | Good |
| pH stability range | 3–11 | 4–10 | 5–10 | 3–11 | 4–10 |
| Caking tendency | Very low | Low | Moderate | Moderate | High |
| Regulatory acceptance | Global | Global | Global | Global | Global |
| Cost efficiency | High | Moderate | Moderate | Moderate | High |
The overall picture is clear. MCC/CMC co-processed systems lead on every performance parameter that directly affects patient experience and clinical reliability — suspension efficiency, sedimentation control, redispersibility, and mouthfeel. Where cost drives formulation and API density is low, formulators may choose sodium CMC alone or HPMC. However, when performance is the priority — as it always should be in regulated pharmaceutical oral suspension development — MCC/CMC sets the benchmark for all alternatives.
These performance results explain why developers increasingly select MCC/CMC as the preferred suspending agent for oral suspensions worldwide.
MCC suspension stabilizer systems dramatically reduce sedimentation rate compared to viscosity-based alternatives. The colloidal network mechanism maintains insoluble particles in uniform distribution throughout the product’s shelf life — ensuring consistent drug content per dose from the first dose to the last.
This is particularly critical in antibiotic oral suspension formulation, where high API loading and particle density create extreme sedimentation challenges. Formulators routinely use MCC/CMC systems in amoxicillin, azithromycin, and cephalosporin suspensions because they effectively handle high-density, high-concentration particle systems, and because these systems often defeat conventional thickeners.
Even after extended storage, microcrystalline cellulose oral suspension formulations typically redisperse to homogeneity within 5–10 seconds of gentle manual shaking. This performance characteristic directly supports dosing accuracy and patient compliance, and it also serves as a key parameter during suspension stability testing in accordance with ICH guidelines.
Formulators find that hard cake formation — the failure mode in which settled particles consolidate into a dense, non-redispersible mass — is virtually eliminated in well-designed MCC/CMC suspension systems.
MCC produces a smooth, creamy suspension texture that is consistently preferred over the slimy or overly viscous textures produced by many competing stabilizer systems. In pediatric oral suspension development, where palatability studies are a regulatory requirement under EMA Pediatric guidelines and FDA PREA, this sensory advantage translates directly into improved compliance and clinical outcomes.
Because MCC is non-ionic and chemically inert, it demonstrates excellent compatibility with the wide range of APIs formulated as oral suspensions:
One of the major advantages of MCC is its measurable contribution to suspension stability improvement across different API classes.
Unlike ionic stabilizers (sodium alginate, certain CMC grades at high concentrations), MCC does not engage in ion-exchange interactions with charged API molecules — eliminating a major source of compatibility failures in oral liquid suspension excipient selection.As a non-ionic oral liquid suspension excipient, MCC demonstrates compatibility with a wide range of APIs and preservatives.
MCC-based pharmaceutical suspension stabilizer systems are compatible with standard pharmaceutical liquid manufacturing equipment and processes. They hydrate readily at room temperature, require no special mixing conditions, and are compatible with common preservation systems (sodium benzoate, potassium sorbate, parabens) and flavoring agents used in pediatric oral suspension formulation.
Microcrystalline cellulose co-processed with carboxymethylcellulose sodium (MCC/CMC) is among the most widely used suspending agents in oral liquid formulation. Its colloidal network structure provides reliable viscosity, sedimentation control, and redispersibility across a broad range of suspension types. Achieving consistent performance, however, depends on careful attention to use level selection, hydration, mixing, pH management, API incorporation, and long-term stability evaluation. The following guidelines address each of these factors in sequence.
The appropriate concentration of MCC/CMC varies with the physical demands of the formulation. Higher-density or higher-loaded systems require a more robust colloidal network and therefore call for higher use levels.
| Suspension Type | Recommended MCC/CMC Level |
|---|---|
| Standard oral suspension | 0.5–1.0% w/v |
| High-density API suspension | 1.0–1.5% w/v |
| High-load antibiotic suspension | 1.0–2.0% w/v |
| Reconstitutable dry suspension | 1.5–2.0% w/w (dry blend) |
| Nutritional / antacid suspension | 0.5–1.5% w/v |
pH optimization: Adjust pH before adding MCC/CMC where possible. Target pH 4.0–7.0 for most oral suspension applications. MCC/CMC performance is stable across this range; extreme acidic or alkaline conditions reduce network integrity.
API incorporation: Add micronized API to the hydrated MCC/CMC vehicle under moderate mixing. Ensure complete wetting before finalizing viscosity adjustment.
Stability evaluation: Conduct accelerated stability testing at 25°C/60% RH and 40°C/75% RH per ICH Q1A. Key parameters: sedimentation volume ratio, redispersibility (shake cycles to homogeneity), viscosity at t=0, 3, 6, 12 months.
These ranges serve as starting points for formulation screening. The target use level within a given range should be confirmed through sedimentation and redispersibility testing, as over-use can produce excessive viscosity that compromises pourability and dose uniformity, while under-use leads to inadequate network integrity and rapid settling.
Full hydration of MCC/CMC before any other processing step is the single most critical requirement for achieving optimal suspension performance. MCC/CMC should be added directly to purified water under moderate agitation, then allowed a minimum of 20–30 minutes of uninterrupted hydration before any APIs or additional excipients are introduced.
Incomplete hydration is a common root cause of formulation failures: an under-hydrated colloidal network cannot develop full yield stress, leading to poor sedimentation control and inconsistent viscosity. In practice, the hydration endpoint can be monitored visually — the dispersion should appear uniformly translucent or slightly opaque with no undissolved particulates — and confirmed by viscosity measurement against a pre-established specification for the hydrated vehicle.
For reconstitutable dry suspensions, MCC/CMC is incorporated into the dry blend during manufacturing, and hydration occurs during the reconstitution step at the point of dispensing. In these cases, the particle size of the dry MCC/CMC and the reconstitution instructions (water volume, shaking protocol) should be validated to ensure complete hydration within a reasonable and practical time frame.
Once MCC/CMC is fully hydrated, mixing speed and equipment geometry must be carefully controlled throughout subsequent processing. Moderate-speed mixing at 300–600 rpm with an appropriate impeller geometry is the recommended operating range.
The colloidal network structure responsible for MCC/CMC’s suspending function is shear-sensitive. High-shear mixing — whether from excessive rotor speed, inappropriate impeller selection, or prolonged processing — can irreversibly disrupt the network, resulting in a permanent loss of viscosity and suspension stability that cannot be recovered by further processing. Anchor or paddle impellers are generally preferred over high-shear dispersers or rotor-stator homogenizers for the main mixing step.
Where high-shear equipment is required for API wetting or particle size reduction, it should be applied before the MCC/CMC vehicle is introduced, or confined to a sub-process in which the API is pre-wetted separately and subsequently combined with the hydrated vehicle under gentle mixing.
The pH of the aqueous phase directly affects the integrity of the MCC/CMC colloidal network and should be adjusted to the target value before MCC/CMC is added, where the formulation process permits. The recommended operating range for most oral suspension applications is pH 4.0–7.0, within which MCC/CMC performance is stable and predictable.
Outside this range, network integrity becomes progressively compromised: strongly acidic conditions (pH < 3) can promote hydrolysis of the CMC component, while highly alkaline conditions (pH > 8) disrupt electrostatic interactions that contribute to network structure. Both extremes result in reduced viscosity and sedimentation control over time.
When the formulation contains pH-sensitive APIs or buffers that interact with CMC, compatibility should be evaluated during early development. Certain multivalent cations — particularly calcium, magnesium, and aluminum — can form ionic cross-links with the carboxymethyl groups of CMC, leading to gel formation or precipitation, and their presence should be identified and managed during excipient screening.
Active pharmaceutical ingredients are incorporated into a fully hydrated, pH-adjusted MCC/CMC vehicle under moderate mixing conditions. Formulators strongly recommend API micronization for poorly soluble compounds because smaller particle size reduces sedimentation rate (Stokes’ law), improves dose uniformity, and enhances wettability.
APIs are added as either a pre-wetted slurry or a fine powder while mixing is maintained at the lower end of the recommended speed range. Complete wetting of all API particles must be achieved before the viscosity is finalized or before the batch moves to the next processing step. Formulators confirm full wetting by ensuring there are no floating aggregates or dry clumps in the system.
If wetting is incomplete at this stage, the system can develop aggregation, dose non-uniformity, and inconsistent redispersibility in the final product.
Excipients that compete with MCC/CMC for water, or that interact with the CMC polymer — such as certain electrolytes, high-concentration surfactants, or water-miscible solvents — are added only after the MCC/CMC network is fully established. Formulators then evaluate their impact on final viscosity and overall stability before finalizing the formulation.
Stability evaluation should follow the ICH Q1A framework, with accelerated storage conditions at 25°C/60% RH and 40°C/75% RH. For oral suspensions, the core physical stability parameters to monitor are as follows:
Viscosity and sedimentation data together provide the most sensitive early indicators of MCC/CMC network degradation. Formulations exhibiting more than a 20% decline in viscosity or a sedimentation volume ratio below 0.9 at any accelerated condition time point should be investigated for root cause before proceeding to long-term storage commitments.
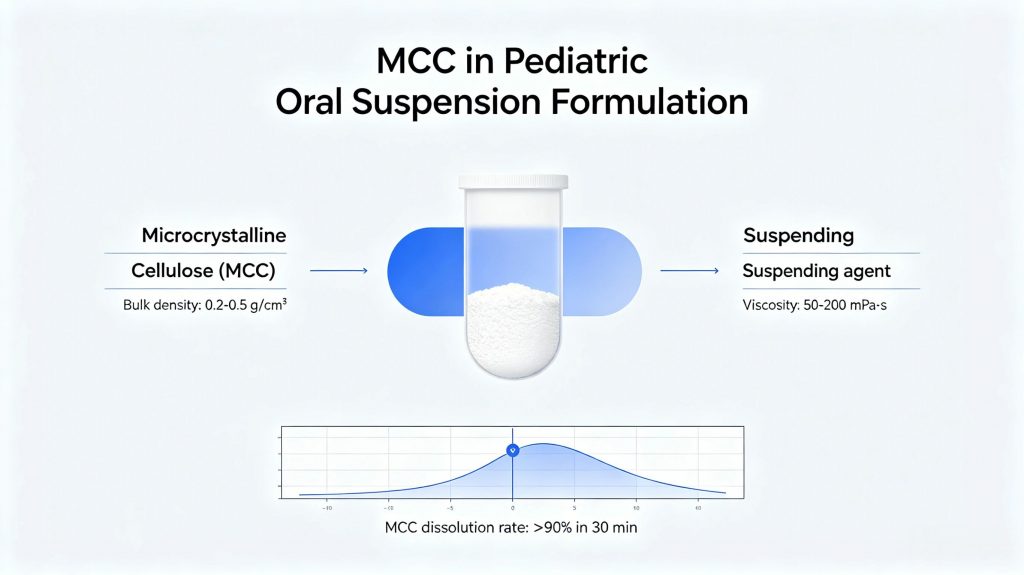
Pediatric oral suspension formulation represents the highest-growth segment for MCC suspension stabilizer applications — and the reasons go beyond simple market size. Children cannot swallow tablets or capsules reliably, particularly below the age of six. Oral liquid suspensions are frequently the only clinically viable dosage form for this population. Yet the performance requirements placed on pediatric suspensions are, in many respects, more demanding than those for adult solid dosage forms.Most leading pediatric formulations rely on an MCC CMC suspension system to ensure dose consistency throughout use.MCC in Oral Suspensions is particularly valuable in pediatric medicines because accurate dose delivery is essential.
Pediatric dosing is weight-based. A 12 kg toddler receiving amoxicillin at 40 mg/kg/day requires a precisely measured, accurately concentrated dose every eight hours. If the suspension has settled unevenly — with API-depleted liquid near the top and drug-concentrated sediment at the bottom — the actual dose delivered may bear little resemblance to the intended dose. Unlike adult patients who may tolerate modest dose variability, young children have narrow therapeutic windows, lower body weight buffers, and immature renal and hepatic clearance mechanisms that make both under-dosing and over-dosing clinically significant.
This is why the performance bar for suspending agents in pediatric formulations is higher than in any other oral liquid application — and why MCC/CMC colloidal suspension systems have become the stabilizer of choice for the most demanding pediatric products on the market.
In adult pharmaceutical formulations, mouthfeel is a quality-of-life consideration. In pediatric formulations, it is a compliance determinant. A child who finds a medication unpleasant will refuse it — consistently, persistently, and regardless of parental instruction. Caregiver frustration, incomplete treatment courses, and therapeutic failure follow directly.
The sensory properties of a pediatric suspension therefore function as a clinical performance parameter rather than a cosmetic feature. Regulatory agencies recognize this shift: both EMA and FDA require palatability assessment during pediatric formulation development, and reviewers evaluate palatability study data as part of the pediatric submission package.
MCC/CMC suspension systems produce a smooth, creamy texture that patients and caregivers consistently prefer over the slimy texture associated with xanthan gum-based systems and the thick, gummy texture of alginate-based formulations.
This sensory advantage is not marginal. In controlled pediatric palatability studies, formulators consistently observe that texture becomes the primary driver of medication acceptance or rejection, even ahead of taste and smell.
Therefore, selecting MCC as the suspension stabilizer directly supports treatment compliance and improves real-world dosing adherence.
Antibiotic oral suspension formulation represents the largest commercial application of MCC/CMC technology worldwide. MCC in Oral Suspensions plays a critical role in stabilizing high-load antibiotic formulations.High API loading, elevated particle density, chemical instability in aqueous environments, and the reconstitution requirements of dry powder systems all combine to create formulation complexity that viscosity-based stabilizers cannot adequately address.
MCC/CMC co-processed systems handle high particle loading at high density without requiring viscosity levels that compromise pourability or mouthfeel.
Their compatibility with buffering systems, sweeteners, flavoring agents, and preservatives used in antibiotic suspensions is well established. So formulators can integrate them smoothly into standard pediatric and adult liquid formulations.
As a result, these systems remain the practical first choice for antibiotic suspension development.
Amoxicillin is the world’s most prescribed pediatric oral antibiotic, and its suspension formulation is one of the most technically demanding applications of MCC stabilizer technology.
Formulated at 125 mg/5 mL and 250 mg/5 mL, amoxicillin trihydrate presents high particle density and relatively large primary particle size — producing strong sedimentation forces that defeat viscosity-based systems at acceptable concentrations. The additional challenge is chemical instability in water: amoxicillin degrades rapidly in aqueous solution, requiring a dry powder for reconstitution format with a 7–14 day post-reconstitution shelf life.
MCC/CMC systems address all of this: rapid network formation upon reconstitution, robust particle entrapment at high loading levels, reliable redispersibility between doses, and full compatibility with the flavoring systems needed to mask amoxicillin’s bitter taste.
Azithromycin suspension at 200 mg/5 mL presents a different challenge. Dosed once daily, the suspension sits undisturbed in the refrigerator for approximately 23 hours between each dose. Each time it is retrieved, it must redisperse uniformly with realistic — not vigorous laboratory — shaking.
MCC/CMC systems maintain azithromycin particles in a loose, easily redispersible state throughout the treatment course. The thixotropic network reforms rapidly after shaking, preventing the particle consolidation during prolonged rest periods that produces hard sediment in CMC-only systems.
Cephalosporin suspensions — cephalexin 125/250 mg/5 mL, cefdinir 125 mg/5 mL, cefuroxime axetil — each present distinct challenges. Cefuroxime axetil particles are often microencapsulated for taste masking, producing larger, denser particles with amplified sedimentation tendency. Cefdinir’s characteristic reddish-brown color means any visible settling immediately triggers caregiver concern — making cosmetic suspension uniformity a direct compliance and commercial consideration alongside the clinical one.
MCC/CMC stabilization handles both the physical and visual stability requirements across this chemically diverse antibiotic class.
Most pediatric antibiotic suspensions are manufactured as dry powder for reconstitution (DPR) — keeping API and water separated until the point of dispensing. This format places dual demands on the MCC/CMC stabilizer: it must blend uniformly in the dry powder state, then hydrate rapidly and completely upon water addition to form a stable colloidal network within seconds of realistic shaking.
Co-processed MCC/CMC grades are specifically suited to this requirement. The intimate CMC coating on MCC microfibrils enables faster, more complete hydration than physical blends — a critical advantage when reconstitution mixing energy is limited by real-world pharmacy or home conditions.
Key formulation considerations for DPR systems:
Reconstituted stability — evaluate sedimentation, redispersibility, viscosity, and content uniformity through the full post-reconstitution shelf life per ICH Q1A
Particle size — finer MCC/CMC grades hydrate faster; include particle size in excipient specification
Moisture control — maintain low moisture content in dry blend to prevent premature hydration during storage
Ibuprofen and acetaminophen oral suspensions are two of the highest-volume pediatric pharmaceutical products globally. Families use them widely for fever and pain management.
Consumers buy these products over the counter. They store them at home. And caregivers often administer them without pharmacist supervision. So performance must go beyond clinical requirements and also meet real-world usability needs.
Ibuprofen pediatric suspension (100 mg/5 mL) and acetaminophen pediatric suspension (160 mg/5 mL) both create API loading and density challenges. These challenges require strong suspension stabilization.
These products are used repeatedly over long periods. Caregivers open, recap, and store bottles for weeks. Then they reuse them during the next illness episode.
So the suspension must redisperse easily after long storage. It must also perform under variable temperature and humidity conditions. And it must work with only gentle shaking, even in low-light or stressful situations.
MCC/CMC systems meet these requirements effectively. Their thixotropic network breaks under shaking and rebuilds at rest. This ensures reliable redispersion under realistic use conditions.
The system also provides a smooth mouthfeel. This improves pediatric compliance. In addition, MCC maintains stability across wide pH and temperature ranges. So it supports consistent performance in household storage conditions.
Regulatory requirements for pediatric drug development have changed significantly over the past two decades. Authorities now treat pediatric formulation as a mandatory development component rather than an optional step.
Three major frameworks drive pediatric oral suspension development and increase demand for high-performance stabilizers.
EMA Paediatric Regulation (EC 1901/2006) requires companies to submit a Pediatric Investigation Plan (PIP) for new medicines and new indications. The EMA Paediatric Committee (PDCO) reviews and approves these plans. When developers choose oral suspensions for pediatric use, they must include formulation development, palatability studies, and stability data. These depend directly on suspension performance.
FDA PREA (Pediatric Research Equity Act) requires pediatric studies for eligible drugs and applications. When developers select liquid pediatric formulations, they must include detailed formulation performance data, including stability and redispersibility.
ICH E11(R1) defines global standards for pediatric clinical development. It emphasizes age-appropriate formulations. It also highlights palatability, dosing accuracy, and stability of liquid dosage forms.
Together, these frameworks make pediatric suspension formulation a regulated deliverable. MCC/CMC systems support these requirements effectively. They improve dosing accuracy, redispersibility, and mouthfeel. So they help developers meet regulatory expectations more reliably.
Using MCC-based suspension systems therefore supports not only formulation quality but also regulatory success across FDA, EMA, and ICH-aligned markets.
Pharmaceutical-grade MCC/CMC holds broad regulatory acceptance across major global markets. Its long history of safe use in oral liquids reduces excipient justification requirements in new submissions.
MCC also remains one of the most widely accepted suspension excipients worldwide.
USP-NF monographs define standards for microcrystalline cellulose used in oral dosage forms. These include identity, purity, viscosity, and microbial limits.
MCC meets these USP-NF requirements. So formulators use it as a baseline-compliant excipient for US submissions.
The European Pharmacopoeia (Ph. Eur.) includes monographs for microcrystalline cellulose and carmellose sodium (CMC). These standards apply across EU member states and other EP-recognized regions.
EP-compliant MCC/CMC supports EMA submissions and national EU registrations.
The Japanese Pharmacopoeia (JP) includes MCC monographs for pharmaceutical use. JP compliance supports submissions to PMDA and Japanese market approval.
Suppliers targeting Japan ensure JP alignment in their documentation packages.
MCC appears widely in the FDA Inactive Ingredient Database (IID) for oral liquids. The database lists established usage levels from approved products.
Formulators use IID data to define safe concentration ranges. This reduces regulatory risk during NDA or ANDA submissions.
Global Regulatory Acceptance
MCC/CMC is accepted in Health Canada, TGA (Australia), ANVISA (Brazil), and most ICH-aligned systems.
This broad acceptance allows developers to use a single MCC/CMC-based formulation across multiple markets. So it reduces redevelopment effort and supports faster global filings.
Oral suspension dosage forms are gaining renewed interest due to demographic shifts, regulatory expansion, and market demand.
Several growth drivers are reshaping suspension development. And each driver increases demand for better stabilizer systems.
Future excipient development will focus on improving suspension stability. And it will maintain patient-friendly rheology.
The future of MCC in oral suspensions is closely linked to the growth of pediatric medicines and ready-to-use liquid formulations.
Regulatory mandates under FDA PREA and EMA Paediatric Regulation have made pediatric formulation development a non-optional component of drug registration strategy for most new chemical entities. As the pipeline of products requiring age-appropriate liquid formulations continues to expand, demand for validated, pharmacopoeially compliant suspension systems is growing in parallel. Palatability, dosing precision, and long-term physical stability — all of which are directly influenced by suspending agent selection — are becoming competitive differentiators in pediatric product development, not merely regulatory checkboxes.
Patient convenience and adherence are pushing a shift toward ready-to-use (RTU) liquid suspensions. This trend is strongest in chronic therapies and home-care use.
RTU systems remove the reconstitution step. So they increase usability and reduce dosing errors. But they also increase stability demands.
The colloidal network must stay stable for 18–24 months. It must control sedimentation over long storage. And it must keep redispersibility after repeated use.
This drives higher use of advanced MCC/CMC systems. Formulators also adopt co-processed grades. These systems improve network strength and long-term durability.
High-dose oral therapies are becoming more common. This includes oncology supportive care, infectious diseases, and metabolic treatments.
These products carry higher API loads than traditional suspensions. So they increase stress on the suspension system.
Formulators must balance viscosity and pourability. At the same time, they must control sedimentation from dense particles.
This pushes development toward tailored MCC/CMC ratios. It also increases use of combination systems.
In addition, formulators use particle engineering. They reduce API particle size. And they lower effective density differences. These steps help maintain stability and bioavailability together.
The nutraceutical market is rapidly expanding suspension formats. These include vitamins, minerals, omega-3s, probiotics, and botanical extracts.
Consumers prefer liquid forms for easier intake. And suspensions often improve absorption compared to solid forms.
However, these products must also meet clean-label expectations. So formulators limit excipients and avoid complex synthetic systems.
MCC/CMC is a strong fit for this segment. It has a natural origin and good safety profile. It also gives stable suspension behavior and smooth mouthfeel.
So it is widely used in nutraceutical liquid systems where both stability and consumer perception matter.
Veterinary medicine is becoming more regulated and more advanced.This shift is driven by EMA Regulation (EU 2019/6) and increased FDA CVM oversight.
Oral suspensions are widely used across companion animals, livestock, and aquaculture.
These products must perform across a wide range of body weights and dosing volumes. They must also meet species-specific palatability requirements.
So formulators require stabilizer systems that are both flexible and robust.
MCC/CMC grades with broad pH stability are preferred. They also maintain performance across temperature variations.
As a result, formulators increasingly adopt these systems in global veterinary suspension development programs.
| Formulation Type | Recommended MCC System |
|---|
| Pediatric Suspension | MCC/CMC |
| Antibiotic Suspension | MCC/CMC |
| Antacid Suspension | MCC/CMC |
| Nutritional Suspension | MCC/CMC |
| Veterinary Suspension | MCC/CMC |
| High Density API | High Strength MCC/CMC |
| Formulation Scenario | MCC Recommended? |
|---|---|
| Pediatric antibiotic suspension | ✓✓ Strongly recommended |
| High-density API (>1.5 g/cm³) | ✓✓ Strongly recommended |
| Reconstitutable dry powder suspension | ✓✓ Strongly recommended |
| Antacid suspension | ✓ Recommended |
| Nutritional oral liquid | ✓ Recommended |
| Low-density API, low loading | Consider vs. HPMC |
| Clear solution (no insoluble particles) | Not applicable |
The same colloidal stabilization technology used in MCC oral suspension systems is also widely applied in pharmaceutical excipients for tablet manufacturing, direct compression systems, controlled-release formulations, and liquid dosage forms.
Microcrystalline Cellulose (MCC)
Hydroxypropyl Methylcellulose (HPMC)

MCC functions as a colloidal suspending agent and physical stabilizer. It forms a three-dimensional gel network that prevents sedimentation, improves redispersibility, and maintains uniform drug distribution throughout the suspension’s shelf life.
MCC provides the structural colloidal network; CMC provides hydration and viscosity. Together, they create a synergistic suspension system that outperforms either component alone — delivering better stability, smoother mouthfeel, and lower sedimentation rates.
Yes — MCC is one of the preferred stabilizers for pediatric suspensions. It delivers dosing accuracy, smooth mouthfeel, compatibility with flavoring and sweetening agents, and excellent redispersibility after storage.
In most pharmaceutical suspension applications, MCC/CMC systems provide superior redispersibility and significantly better mouthfeel compared to xanthan gum. Xanthan gum produces noticeable sliminess at the concentrations needed for effective suspension — a sensory disadvantage MCC avoids through its colloidal mechanism.
Most formulations use 0.5–2.0% w/v MCC/CMC suspension system, depending on API particle density, target viscosity, and intended shelf life. High-density APIs and reconstitutable antibiotic suspensions typically require the higher end of this range.
Avicel RC-591 (FMC BioPolymer) has long served as the reference-standard co-processed MCC/CMC grade for oral suspension formulation. ACTA-591 functions as the primary alternative, sharing approximately 89% microcrystalline cellulose and 11% carboxymethylcellulose sodium. ACTA-591 matches the colloidal network structure, viscosity profile, and suspension performance of RC-591. It also comes with the pharmacopoeial compliance documentation (USP-NF, EP, JP) required for pharmaceutical submissions. Formulators switching from RC-591 to ACTA-591 should perform head-to-head functional comparability tests — including viscosity, sedimentation volume ratio, and accelerated stability — in the actual product formulation before finalizing the substitution.
MCC/CMC works with most antibiotic classes used in oral suspension formulations, including penicillins, cephalosporins, macrolides, and fluoroquinolones. Antibiotic oral suspensions — such as amoxicillin, amoxicillin-clavulanate, azithromycin, and cefuroxime axetil — represent some of the highest-volume commercial uses of MCC/CMC suspension technology. However, compatibility varies and must be assessed case by case. Formulators must consider the API’s ionic character (highly cationic compounds may interact with the anionic CMC), the target pH, and the presence of multivalent metal ions in certain antibiotic salts, which can cross-link CMC chains and alter network viscosity. They should conduct compatibility screening covering physical appearance, viscosity retention, and API assay under both ambient and accelerated storage conditions during early development.
MCC/CMC improves redispersibility by forming a thixotropic, structured colloidal network upon hydration. MCC particles create a three-dimensional network that traps API particles and prevents hard caking. When shear occurs during pouring or shaking, the network breaks down and allows free flow. Once shear stops, the network quickly rebuilds, re-entrapping the API uniformly. This thixotropic recovery keeps the settled sediment soft and loosely structured, requiring only gentle shaking to resuspend. Without an effective network, API particles consolidate into a hard cake that cannot be resuspended normally, causing dose inconsistency.
At typical oral suspension concentrations (0.5–2.0% w/v), MCC/CMC does not significantly affect drug release for most APIs. Oral suspensions already present fine, pre-wetted API particles in an aqueous medium, minimizing dissolution barriers. The colloidal network stabilizes the suspension physically without forming a persistent diffusion barrier. For highly lipophilic or poorly soluble APIs, high MCC/CMC levels may slow API transfer to the gastrointestinal membrane. In these cases, formulators should conduct in vitro dissolution testing and, if necessary, comparative bioavailability studies to ensure the intended pharmacokinetic profile. Drug release concerns mainly arise in solid modified-release matrices, not in liquid suspensions.
MCC/CMC performs best in oral suspensions at pH 4.0–7.0. Within this range, the colloidal network maintains viscosity, gel strength, and suspension stability over shelf life. Below pH 3, acid-catalyzed hydrolysis can degrade MCC and reduce network integrity. Above pH 8, CMC conformational changes weaken electrostatic interactions, causing viscosity loss. Formulators creating suspensions outside pH 4.0–7.0 — such as antacids or highly buffered antibiotics — should confirm compatibility through accelerated stability tests, focusing on viscosity retention and sedimentation behavior.
An MCC CMC suspension system combines microcrystalline cellulose and sodium carboxymethyl cellulose. It forms a structured colloidal network that enhances suspension stability, redispersibility, and mouthfeel in pharmaceutical liquids.
MCC/CMC stands out as one of the most effective suspending agents for oral suspensions. It delivers excellent sedimentation control, ensures easy redispersion, and provides a patient-friendly mouthfeel.
MCC in Oral Suspensions is more than an excipient application—it is a complete formulation strategy for achieving long-term suspension stability.The colloidal network mechanism that MCC/CMC systems deploy addresses the fundamental physics of particle sedimentation in a way that viscosity-based thickeners cannot replicate. The result is measurably better suspension stability, dramatically improved redispersibility, superior mouthfeel, and the dosing accuracy that patients — especially pediatric patients — depend on.For any modern antibiotic oral suspension formulation, MCC/CMC remains one of the most reliable stabilization technologies available.
As pharmaceutical development continues to prioritize patient-centric dosage forms, age-appropriate formulations, and oral liquid systems for special populations, demand for high-performance microcrystalline cellulose oral suspension stabilizer systems will continue to grow. Formulators who understand MCC’s mechanism and use it correctly will consistently produce better suspension products — and bring them to market faster.
At Acta Biotechnology, we supply pharmaceutical-grade MCC and MCC/CMC suspension systems with full pharmacopoeial compliance, technical formulation support, and the supply reliability that commercial pharmaceutical manufacturing demands.
Looking for a reliable MCC suspension stabilizer supplier?
Acta Biotechnology provides pharmaceutical-grade MCC and MCC/CMC suspension systems with USP/EP/JP compliance, technical formulation support, and stable global supply.
Contact our technical team to discuss your oral suspension formulation project, request samples, or obtain customized recommendations for pediatric, antibiotic, nutraceutical, and veterinary suspension products.